After an Achilles tendon rupture, heel height is not a fashion detail — it is how clinicians control strain on the healing repair. Whether that comes from heel wedges in a walking boot, a hinge angle, or lifts in your shoes after the boot, the goal is the same: keep the tendon from healing over-stretched while you gradually load it again.
This article explains why heel height matters, what the evidence says for heel lifts (including after rupture and in tendinopathy research), and how to think about boot progression, footwear, and long-term strength.
Contents
- Key takeaways
- Why heel height matters
- Evidence on heel lifts and tendon load
- Heel height in surgical vs non-surgical care
- Boot phase, video overview, and practical numbers
- Long-term effects and footwear transition
- What this means for your recovery
- Frequently asked questions
- References
Key takeaways
- Heel height controls tension on the healing tendon — especially while the repair is still “easy to stretch.”
- Small heel lifts are commonly used when moving from boot to shoes; many protocols use around 0.5–1 cm in both feet at first, then wean — follow your team, not a rigid calendar you found online.
- Boot wedge or hinge changes should match your protocol; see Achilles boot wedge removal for why rushing is risky.
- Tendon elongation (healing long) is linked to weaker push-off and lower heel-rise for some people — it may not hurt much at the time, but it can matter later.
- Do not chase aggressive calf stretching early; guidance varies, but many teams avoid forceful dorsiflexion stretches for a long time after rupture — see foot position after rupture.
- Boot brand matters less than compliance; if you are choosing equipment, Aircast vs VACOped compares how each device achieves angle.
Why heel height matters
Reduced tendon strain while walking
Raising the heel shortens the muscle–tendon unit slightly and reduces tensile load on the Achilles during gait. In mid-portion Achilles tendinopathy (painful tendon without a fresh rupture), trials have used ~12 mm in-shoe lifts as an intervention — a useful biomechanical proof-of-concept, even though tendinopathy is not the same problem as an acute rupture.
Elongation, heel-rise, and power
After rupture, tendon length and heel-rise performance are important long-term markers. Research using imaging and strength testing has linked greater tendon elongation and larger side-to-side heel-rise deficits to functional limitations for some patients. That is why “tip-toe” protection in early healing and careful progression out of heel lift later matter.
Heel-rise height, repetitions, and total work correlate with practical measures such as walking speed and ankle power — reasons clinicians track them in clinic, not to obsess over gym stats.
Evidence on heel lifts and tendon load
HEALTHY trial (heel lifts vs eccentric exercise in tendinopathy)
The HEALTHY trial randomised adults with mid-portion Achilles tendinopathy to 12 mm prefabricated heel lifts versus a calf eccentric exercise programme. At 12 weeks, mean VISA-A scores improved by 26.0 points in the heel lift group versus 17.4 in the exercise group — favouring heel lifts on average, though the authors noted uncertainty around whether the difference always crosses the threshold patients would notice day to day.
The quoted conclusion in the paper:
In adults with mid-portion Achilles tendinopathy, heel lifts were more effective than calf muscle eccentric exercise in reducing pain and improving function at 12 weeks.
How to use this evidence fairly: it supports heel elevation as a plausible load-management tool in tendinopathy. For acute rupture, decisions are different (immobilisation / boot angles / surgery choices), but the principle — managing dorsiflexion strain — is shared.
What rupture-specific imaging studies add
Separate literature on Achilles rupture uses measures such as the Achilles tendon resting angle (ATRA) and compares side-to-side heel-rise work. Those papers help explain why teams are cautious about sudden loss of heel height (for example jumping straight into flat shoes after weeks in a boot).
Heel height in surgical vs non-surgical care
Non-surgical treatment is first-line for many acute ruptures when the pattern fits standard criteria — surgery is reserved for specific situations your team will explain (for nuance, see surgery vs non-surgical outcomes).
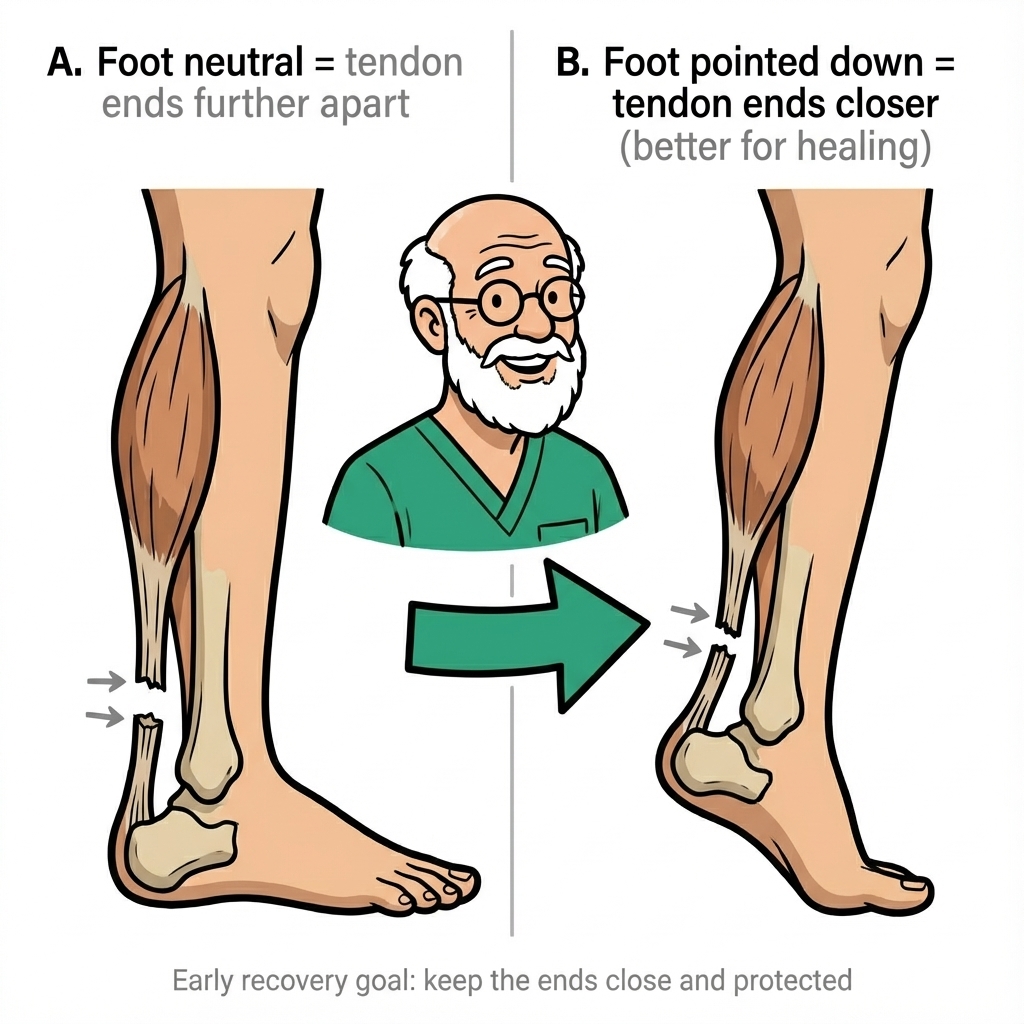
Either way, early protection usually means keeping the ankle plantarflexed (“toes down”) so torn ends sit closer while the first bridge forms. Preventing elongation remains important even after a surgical repair — hardware does not remove the need for careful positioning and progression.
Boot phase, video overview, and practical numbers
If you prefer a visual overview of pain management ideas around heel lifts (general education), this external video may help — it is not a substitute for your own protocol:
Boot angles and wedge schedules
Early on, many protocols aim for roughly ~30° plantarflexion in a walking boot, then reduce angle in steps via heel wedges or a hinged boot. Typical first wedge changes sometimes begin from around week 5 for some pathways — but your orthopaedic or fracture clinic rules win.
Most teams plan boot weaning around weeks 10–12, criteria-based, with gradual time out of the boot — not a single “free day” out of nowhere. That lines up with how modern rehabilitation balances protection and loading.
After the boot: heel lifts in shoes
Once you are cleared for shoes, flat ballet-style footwear is usually a bad first step — the ankle can dorsiflex more than the young repair tolerates. Many protocols use a small lift in both shoes for symmetry:
| Phase or situation | Typical heel-height thinking (examples only) |
|---|---|
| In boot (early) | Strong plantarflexion — often ~30° depending on boot/settings |
| Post-boot transition | Small lift both feet — many protocols ~0.5–1 cm initially |
| Insertional tendinopathy (different condition) | Sometimes higher temporary lifts are used in trials — rupture care follows different rules |
| Return toward normal shoes | Gradually lower lift and/or use shoe drop as strength allows |
Education resources vary: some institutions publish example numbers (for example ~6 mm lifts) as illustrations, not prescriptions — treat them as conversation starters with your clinician, not checkboxes.
Boots, inserts, and brands
Aircast-style boots usually use stacked heel wedges; VACOped uses an adjustable hinge. Both can produce excellent outcomes when protocol adherence is strong — see Aircast vs VACOped.
At night, if the boot is unbearable, ask about a night splint that holds a safe angle — many patients sleep better than in a heavy walker; see our Achilles night splint page.
Balancing protection vs calf shortening
Long periods in plantarflexion can contribute to stiffness and muscle shortening, while removing height too fast can reload elongation risk. That tension is why progression should be stepwise and supervised, with checks on pain, swelling, gait quality, and simple strength tests your team prefers.
Long-term effects and footwear
Elongation and re-rupture
Re-rupture is uncommon (about 3–5% in modern series) but serious — usually linked to loss of protection or big mistakes in load, not to choosing “12 mm vs 10 mm” on one idle afternoon. Elongation is a separate but meaningful problem: it can leave you functional, yet weaker on push-off than you might have been with tidier length.
Researchers including Silbernagel have emphasised that minimising elongation and regaining heel-rise ability may matter for demanding activities long term.
Shoes after the boot
Around the time teams start weaning the boot — often in that week 10–12 window, individually — you may hear advice to favour higher-drop shoes first and to avoid suddenly living in flat, flexible shoes. Adding a modest orthotic lift on top of a ~10 mm running-shoe offset is a common example of how clinicians dampen dorsiflexion moment in early shoe walking.
Calf “tightness” after rupture is common; aggressive stretching is not the same thing as safe loading. Many protocols delay forceful dorsiflexion stretching until much later tendon maturation — sometimes 12+ months — and your clinician should set that pace.
For week-by-week context, Achilles rupture timeline and torn Achilles recovery are the home-base FAQs on this site.
What this means for your recovery
Practical priorities:
- Treat wedge / hinge / lift changes like medication — do not improvise faster progress because walking feels fine; comfort does not equal mature tendon strength (boot wedge article).
- Use symmetry — if you lift one side, many teams lift both early on to avoid limp and back issues.
- Plan sleep — unprotected dorsiflexion at night undoes good daytime habits; consider a night splint (splint hub).
- Know clot symptoms during immobilisation — new one-leg swelling, calf pain unlike your injury, breathlessness, or chest pain need urgent advice (blood clot risk after Achilles rupture).
- Rehab is staged — our structured Achilles recovery course walks through what each phase is trying to achieve.
If you are freshly injured, first 24 hours after Achilles rupture is the right “start here” article.
Frequently asked questions
How do I know my heel lift is too high or too low?
Too high often feels unstable or changes your gait; too low may not unload the tendon enough. Many protocols use roughly 12 mm in-shoe lifts when transitioning after a boot, but your clinician should set the height to match your stage. If you get new pain, swelling, or a sense of slipping at the back of the ankle, stop adjusting on your own and ask your team.
When is it safe to start lowering heel wedges or stopping lifts?
Only on your clinician’s schedule. In the boot, wedge or hinge changes are tied to how healing is progressing — not to a good day or a holiday. After the boot, lifts are usually weaned gradually over weeks to months as strength improves. Rushing either step can overload immature tissue.
What shoe heel-to-toe drop is best after I am out of the boot?
Most people are steered toward a higher-drop running-style shoe at first, often with a small heel lift added in both shoes for symmetry — many protocols use something in the 0.5–1 cm range initially, then taper. Zero-drop or minimal shoes come later, if at all, when your tendon and calf are clearly ready.
References
- Rabusin CL, Menz HB, McClelland JA, et al. Efficacy of heel lifts versus calf muscle eccentric exercise for mid-portion Achilles tendinopathy (HEALTHY): a randomised trial. Br J Sports Med. 2021;55(9):486-493. PubMed
- Silbernagel KG, Steele R, Manal K. Deficits in Heel-Rise Height and Achilles Tendon Elongation Occur in Patients Recovering from an Achilles Tendon Rupture. Am J Sports Med. 2012;40(7):1564-1571. DOI
- Costa ML, et al. Plaster cast versus functional brace for non-surgical treatment of Achilles tendon rupture (UKSTAR): a multicentre randomised controlled trial and economic evaluation. Lancet. 2020;395(10227):441-448. PubMed
- Maempel JF, et al. A Randomized Controlled Trial Comparing Traditional Plaster Cast Rehabilitation With Functional Walking Boot Rehabilitation for Acute Achilles Tendon Ruptures. Am J Sports Med. 2020;48(11):2755-2764. PubMed
Primary source: Rabusin CL, Menz HB, McClelland JA, et al. (2021). Efficacy of heel lifts versus calf muscle eccentric exercise for mid-portion Achilles tendinopathy (HEALTHY): a randomised trial
