If you are in a walking boot after an Achilles rupture, wedge removal (or hinge adjustment) is one of the most important — and most misunderstood — parts of early rehab. The basic idea is simple: your foot usually starts pointed down (plantarflexion) to keep the torn tendon ends close while the first healing bridge forms. Over time, your team gradually brings the ankle toward neutral so the tendon can adapt to a little more length and load without being overstretched too soon.
This article explains why that progression is deliberately slow, what typical timelines look like (with the caveat that your protocol may differ), and why removing wedges too fast is one of the common mistakes patients regret.
Contents
- Key Takeaways
- Why Early Achilles Rehab Starts Toes Down
- What “Wedge Removal” Actually Does
- A Typical Progression (Example Only)
- Why Rushing Wedge Removal Is Risky
- Wedge Boots Versus Hinged Boots
- What This Means for Your Recovery
- Frequently Asked Questions
- References
Key Takeaways
- Gradual wedge removal or hinge adjustment is how clinicians match tendon load to healing stage — the goal is controlled lengthening of the repair, not a race to flat foot
- Early weeks usually prioritise maximum plantarflexion (toes-down posture in the boot) to support tendon end apposition; how long that lasts varies by protocol
- Removing wedges too early — because walking feels easy or you want a “normal” ankle angle — can contribute to tendon elongation (healing “long”), which is linked to weaker push-off and smaller calf long term for some people
- Typical protocols often move the foot toward neutral over roughly weeks 6–10, with boot weaning commonly discussed around weeks 10–12 — but your dates may differ; always follow your team
- Compliance matters more than boot brand; understanding why the schedule exists makes it easier to tolerate slow progress — see Aircast vs VACOped for how different devices achieve angle
- Red-flag symptoms after a change in wedges or hinge settings (new pop, severe pain, instability) need urgent medical review; re-rupture is uncommon (about 3–5%) but serious
Why Early Achilles Rehab Starts Toes Down
After a rupture, the tendon ends need to stay close enough for new tissue to bridge the gap. A toes-down ankle position tends to shorten the distance between ends compared with a neutral or toes-up position — that principle is tendon approximation, which we explain in more detail in foot position after Achilles rupture.
Your boot is not just for walking — it is a positioning system. Whether you use heel wedges or a hinged orthosis, the early phase is usually about protecting that geometry while still allowing protected weight-bearing as your protocol allows.
What “Wedge Removal” Actually Does
Each time you remove a heel wedge or change a hinge setting to allow a less plantarflexed ankle, you increase the dorsiflexion moment on the healing tendon — in plain terms, you ask the repair to tolerate a bit more stretch with every step.
That is not bad; it is necessary for eventually walking with a neutral ankle. The problem is timing: if you add stretch before the tissue can handle it, the healing tendon may creep longer over time.
So wedge removal is really load progression disguised as a simple equipment change.
A Typical Progression (Example Only)
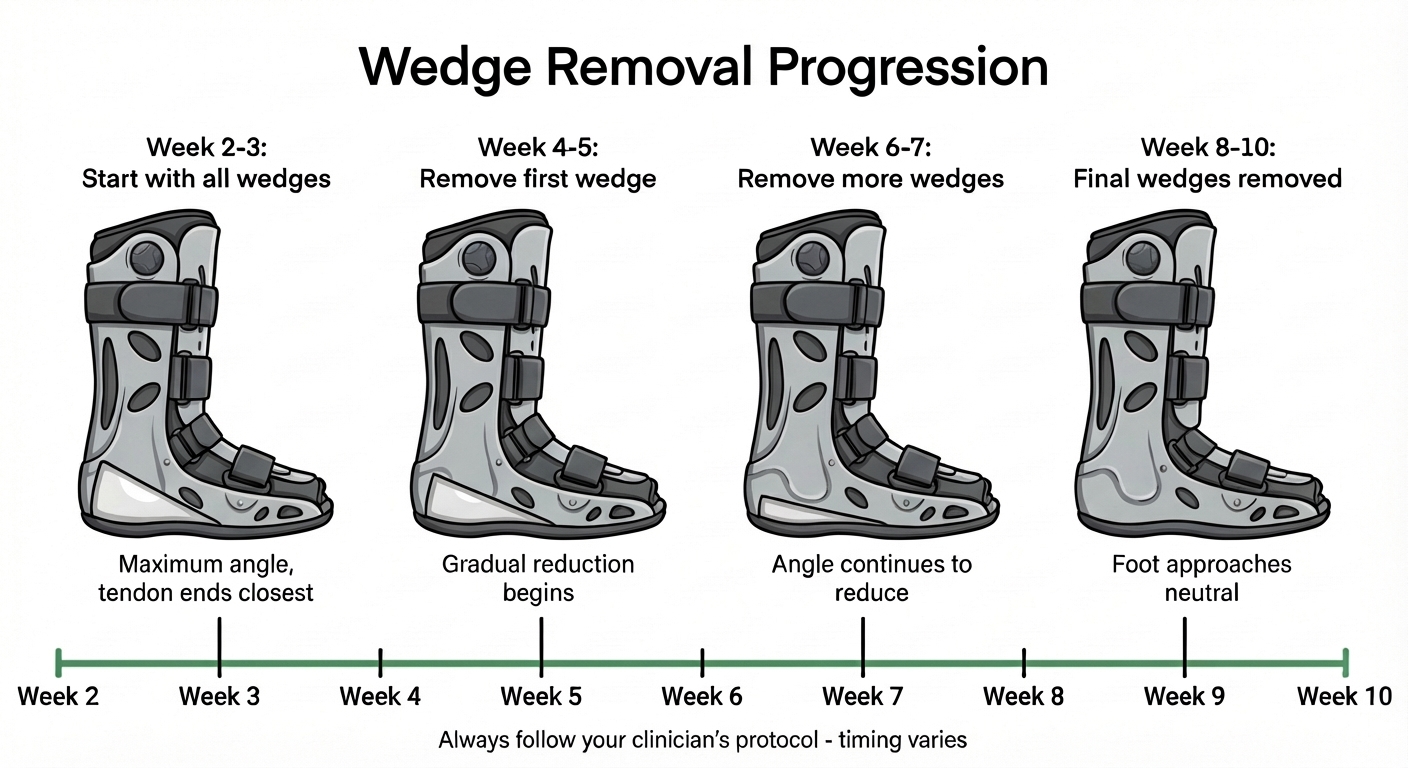
The hero image on this page shows one educational timeline: starting with all wedges in place, then thinning the heel build-up over time, then approaching a flat insole and a more neutral foot position, with a week 2–week 10 scale underneath.
Important: that graphic is not a prescription. Some teams start wedge reduction earlier or later than any example you see online; some use more or fewer wedge steps; some protocols rely mainly on hinge changes instead of inserts.
A broad pattern many patients recognise (still not universal) looks like this:
| Phase | What often happens (examples) | What it is trying to do |
|---|---|---|
| Early protection | Foot held in strong plantarflexion — often no wedge removal yet | Keep tendon ends approximated while the first bridge forms |
| Gradual angle reduction | First wedge out or first hinge step — then further steps spaced out | Let the repair adapt to slightly more tension in a controlled way |
| Approaching neutral | Fewer wedges left, or hinge nearing neutral setting | Prepare the tendon for functional loading without a sudden jump |
| Boot weaning | Transition out of the boot, often weeks 10–12 in many guidelines — criteria-based | Move from boot protection to footwear and rehab exercises |
For how this sits alongside inflammation, bridge building, and remodelling, see Achilles tendon healing and early protection. For week-by-week expectations at a high level, our Achilles rupture timeline FAQ is a useful companion.
Why Rushing Wedge Removal Is Risky
The mistake we hear most often is impatience: a wedge removed “because it felt fine,” or a hinge advanced after a good day, without realising that comfort in the boot does not equal mature tendon strength.
Tendon elongation — healing in a longer, slacker position — is a real clinical concern after Achilles rupture. It may not hurt much at the time, but it can matter later for push-off power and heel-rise height. Research using imaging and follow-up has linked elongation to functional deficits in some patients, which is why modern rehab emphasises gradual progression rather than early aggressive dorsiflexion.
That is the patient-friendly version of gradual load adaptation: give the collagen time to stiffen and remodel before you ramp up stretch.
Wedge Boots Versus Hinged Boots
| Feature | Wedge-style boots (common example: Aircast pathway) | Hinged boots (common example: VACOped pathway) |
|---|---|---|
| How angle changes | Remove heel inserts in steps | Adjust hinge limits in steps |
| What you feel | Heel drops slightly as wedges come out | Angle changes with mechanical settings |
| What you must not do | Skip wedges or remove several at once without approval | Free-style the hinge to neutral early |
Outcomes are generally similar when rehabilitation is taken seriously — large trials comparing casting with functional bracing found comparable long-term function for many people, with early weight-bearing in a brace part of modern care. The lesson for wedge removal is parallel: the schedule matters more than the logo on the boot.
If you are comparing devices or shopping for accessories, the Aircast vs VACOped article goes deeper without pushing one brand as “essential.”
What This Means for Your Recovery
- Treat wedge and hinge changes like medication — do not change the dose because you had a good day
- Ask your team for a written schedule — dates, or “after review at clinic X,” beats guessing from blogs
- Expect odd sensations — a little tightness or awkwardness after a change can happen; unrelenting pain or instability is different — call in
- Plan sleep — rolling into unprotected dorsiflexion at night undermines even perfect daytime wedge discipline; if the boot is unbearable overnight, ask about a night splint that holds a safe angle — see our Achilles night splint page
- Pair patience with structure — our Achilles recovery course is built around the same philosophy: clear rules, gradual loading, no heroics in week two
When to seek urgent help: a new pop or snap, sudden loss of confidence in the leg, severe pain after a slip or stretch, or symptoms that feel like the first rupture — treat as urgent. Re-rupture is uncommon but catastrophic when it happens.
Frequently Asked Questions
Why can’t I remove boot wedges faster if I feel fine?
Feeling comfortable in the boot does not mean the healing tendon is ready for more stretch. Each wedge or hinge step changes how much tension goes through the repair. Removing wedges early can overload immature tissue and contribute to healing in a longer, weaker position (tendon elongation). Your schedule is there to match load to biology — not to how you feel on a single day.
What is the difference between wedge removal and hinge adjustment?
Wedge boots (such as many Aircast-style designs) use stacked heel inserts you remove one at a time to lower the heel and bring the ankle toward neutral. Hinged boots (such as the VACOped) use an adjustable ankle hinge to change the allowed angle in controlled steps. Both aim for the same idea: gradual reduction of plantarflexion — not a sudden jump to a flat ankle.
At what week should my first wedge come out?
There is no single correct week for everyone. Some protocols keep maximum plantarflexion for several weeks before any change; others begin stepping down earlier. The infographic on this page shows one example pattern — your fracture clinic or physiotherapist will give you the dates that match your tear, treatment plan, and local guideline.
What are signs I might be progressing too fast?
New sharp pain at the back of the ankle, a sense of slipping or “giving way,” increasing swelling after a wedge change, or pain that does not settle with elevation and relative rest should prompt you to contact your team before taking the next step. A new pop or snap, or symptoms like the original injury, need urgent assessment.
When do people usually come out of the boot completely?
Many protocols aim for boot weaning around weeks 10–12, but the decision should be criteria-based — how the tendon feels, strength, and your clinician’s examination — not only the calendar. Transition is usually gradual (a little time out of the boot each day, building over one to two weeks), often with heel lifts in shoes at first.
References
-
Willis K, et al. Plaster cast versus functional brace for non-surgical treatment of Achilles tendon rupture (UKSTAR): a multicentre randomised controlled trial and economic evaluation. Lancet. 2020;395(10227):441-448. PubMed
-
Ellison P, Molloy AP, Mason LW. Early Protected Weightbearing for Acute Ruptures of the Achilles Tendon: Do Commonly Used Orthoses Produce the Required Equinus? Foot Ankle Int. 2017;38(11):1300-1305. PubMed
-
Diniz LO, Pacheco FS, Guerra-Pinto F, et al. Achilles tendon elongation after acute rupture: is it a problem? A systematic review. Knee Surg Sports Traumatol Arthrosc. 2020;28(12):3982-3991. DOI
-
Silbernagel KG, Steele R, Manal K. Deficits in Heel-Rise Height and Achilles Tendon Elongation Occur in Patients Recovering from an Achilles Tendon Rupture. Am J Sports Med. 2012;40(7):1564-1571. DOI
-
Qureshi SA, Ibrahim T, Rennie WJ, Furlong AJ. Dynamic Ultrasound Assessment of the Effects of Knee and Ankle Position on Achilles Tendon Apposition Following Acute Rupture. J Bone Joint Surg Am. 2011;93(24):2265-2270. PubMed
Primary source: Willis K, et al. (UKSTAR); The Lancet (2020). Plaster cast versus functional brace for non-surgical treatment of Achilles tendon rupture (UKSTAR): a multicentre randomised controlled trial and economic evaluation
