If you have just ruptured your Achilles tendon, foot position after Achilles rupture is one of the simplest ideas — and one of the most important. Clinicians call the goal tendon approximation: holding the torn ends close enough for healing tissue to bridge the gap. For most people in the emergency phase, that means plantarflexion (foot pointed down, “toes down”), not a relaxed 90-degree ankle.
This article explains why neutral can feel “natural” but work against the tendon early on, how boots and splints hold the safer angle, and what protection really means in the first weeks — without turning it into fear.
Contents
- Key Takeaways
- What Is Tendon Approximation?
- Neutral Versus Toes Down: What Changes
- Why Early Recovery Is About Protection, Not “Testing” the Ankle
- How Boots and Splints Hold the Angle
- What This Means for Your Recovery
- Frequently Asked Questions
- References
Key Takeaways
- Tendon approximation means keeping the torn Achilles ends close while new tissue bridges the gap — plantarflexion (toes down) usually does this best early on
- A neutral ankle (roughly right angle) often increases the gap between ends compared with a protected toes-down position — that is why strict boot or cast angles exist in the first weeks
- Early recovery is not a range-of-motion challenge; it is protection from uncontrolled dorsiflexion (toes up) when tissues are still weak
- Small, repeated unprotected stretches upward can contribute to healing in a longer, slacker tendon — not always obvious on day one, but relevant for push-off strength later
- Your protocol (wedges, hinge settings, weight-bearing rules) is doing biomechanical work for you — follow your team’s schedule; see Aircast vs VACOped for how different boots achieve angle
- Night-time protection matters because the foot can roll into a vulnerable position during sleep — options such as a night splint are worth discussing if the boot is unbearable overnight
What Is Tendon Approximation?
Think of the ruptured tendon ends like two rope ends that need to meet so your body can lay down a healing bridge. If the ends sit far apart, the body still heals — but it may need more scar tissue to span the distance. If the ends are repeatedly pulled apart in the early weeks, the repair can lengthen (sometimes called tendon elongation or healing “long”).
That is the patient-friendly version of approximation: closer ends, more controlled healing geometry — within what your clinician aims for.
For how this fits into inflammation → bridge building → remodelling, see our article on Achilles tendon healing and early protection. The present topic is the positioning that supports that biology.
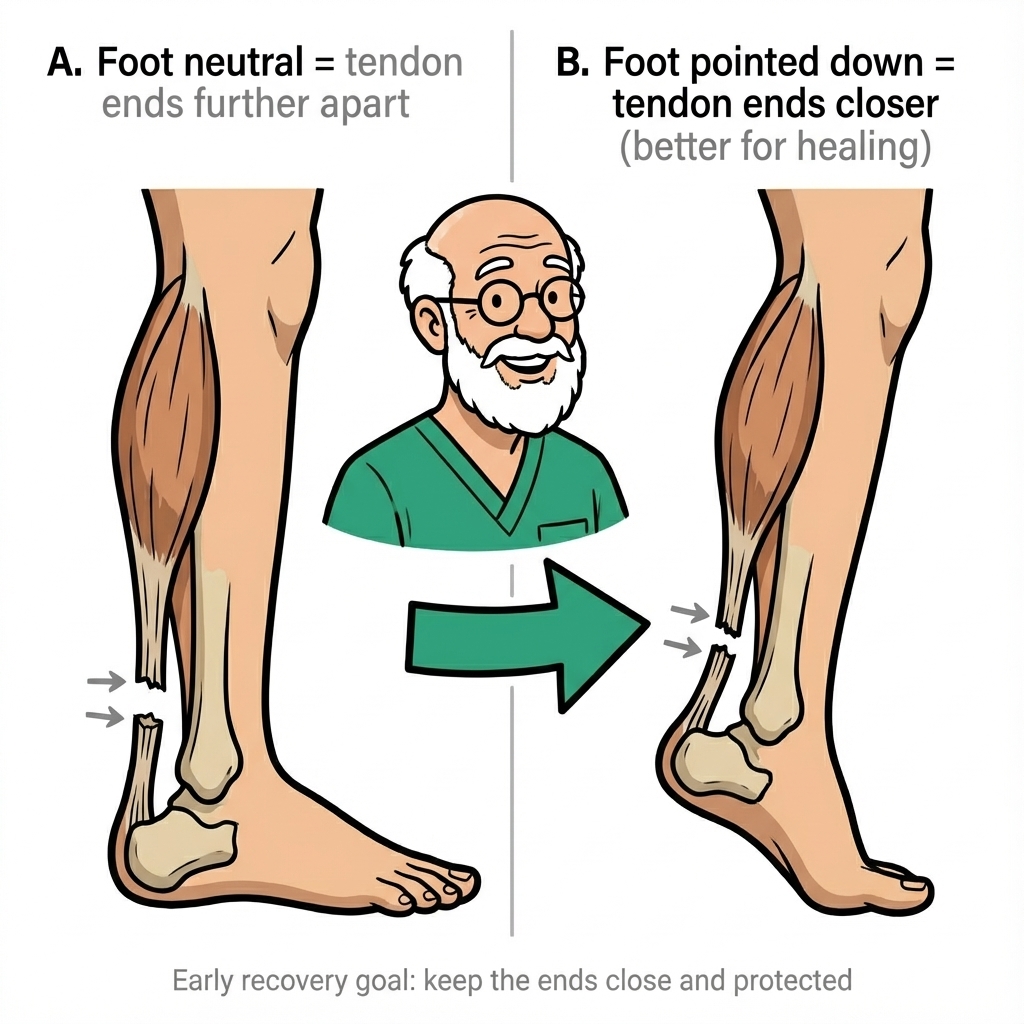
Neutral Versus Toes Down: What Changes
The diagram at the top of this page shows the same idea in pictures: with the foot neutral, the torn ends sit further apart; with the foot pointed down, the ends come closer. That is the clinical reason teams emphasise equinus (toes-down) positioning in the early phase.
| Position | What patients feel | What it tends to do to the gap* |
|---|---|---|
| Plantarflexion (toes down) | Heel loaded, calf shortened, “tip-toe” posture in the boot | Tends to approximate tendon ends |
| Neutral | A “normal” 90-degree ankle can feel comfortable when sitting | Tends to increase separation of ends compared with equinus |
| Dorsiflexion (toes up) | Stretch over the front of the ankle | Tends to open the tear — highest risk when unprotected early on |
*Individual anatomy and tear pattern vary; your team may describe your injury differently.
Laboratory work on cadaveric models and imaging studies reinforces what clinics teach: immobilisation in equinus is associated with smaller gaps than more dorsiflexed positions, and boot set-up changes how much apposition is achieved. Real patients are not cadavers — but the direction of effect is why your angle prescriptions exist.
Why Early Recovery Is About Protection, Not “Testing” the Ankle
It is easy to assume early weeks are for “gentle movement” and curiosity: Can I dorsiflex yet? Can I take a wedge out early because I feel good? In many protocols, early weight-bearing in a boot is encouraged — but that is protected loading, not barefoot stretching.
Protection means:
- Keeping the boot, cast, or splint on according to instructions (often 24/7 early on, including a plan for sleep)
- Avoiding forced upward bending of the ankle outside your allowed range
- Not accelerating wedge removal or hinge changes without clinician approval — see the recovery timeline for how phases typically line up
Aggressive stretching too early is not the goal; most teams delay hard stretching until the tendon is far enough along (often many months). That position matches modern rehab principles: load when protected, do not chase range at the expense of the healing bridge.
How Boots and Splints Hold the Angle
Your walking boot is not fashion — it is a positioning device. Whether you use heel wedges or a hinged orthosis, the job is to keep the ankle in safe equinus and then step down the angle in a controlled way. Imaging-based studies of common boots show real differences in how much ankle plantarflexion is achieved in practice, which is why fitting and follow-up matter.
Practical implications:
- Do not remove wedges early because walking feels easy — each step changes tendon tension
- If you are between brands, outcomes are generally similar when protocols are followed; see Aircast vs VACOped
- If sleep in the boot is unsafe or unbearable, ask about a night splint that holds plantarflexion — rolling into unprotected dorsiflexion is a common pitfall
For structured, week-by-week education (including how rehab ramps up once protection priorities shift), our Achilles recovery course follows the same themes: clear rules, gradual progression, no heroics in week two.
What This Means for Your Recovery
- Treat angle like a prescription — wedges and hinge settings are tied to tendon tension, not comfort alone
- Ask what “neutral” means for you — in clinic language, neutral is not always your friend in week one
- Plan sleep — if the boot slips off or you cannot tolerate it, get a plan rather than “toughing it out” unprotected
- Expect psychological whiplash — understanding why toes-down matters can reduce the urge to “check” the ankle constantly
- Follow your own team if advice differs — countries and surgeons vary; this article explains general principles
When to seek urgent help: a new pop, snap, sudden inability to trust the leg, or severe pain after a specific incident — treat that as urgent; see our note on re-rupture risk (about 3–5%) in the healing phases article.
Frequently Asked Questions
What does tendon approximation mean after an Achilles rupture?
Approximation means bringing the torn tendon ends closer together. In plantarflexion (foot pointed down), the calf and heel relationship tends to shorten the gap between ends. In neutral or dorsiflexion, the gap tends to widen. Your boot or cast holds the angle that your team believes is safest for your tear.
Is a neutral ankle position bad for a fresh Achilles rupture?
Neutral is often a higher-tension posture for a fresh tear than controlled equinus. It is not that a single second at neutral always causes harm — it is that your immobiliser is there to limit how often and how far the ankle drifts into dorsiflexion while tissue is weak.
Why does my team keep saying “toes down” or equinus?
Equinus is the medical term for a toes-down ankle position. It is used because it tends to approximate tendon ends in the early healing phase. How much equinus and for how long is protocol-dependent.
Can small mistakes in foot position really change my outcome?
Perfection is not the standard — people are human. The concern is repeated or forceful dorsiflexion without protection while the bridge tissue is immature. That is the rationale for night protection, careful progression, and not stretching aggressively too soon.
What are warning signs that I need urgent medical review?
A new pop or snap, sudden collapse of confidence in the leg, sharp pain after a twist, or symptoms resembling the original rupture need urgent reassessment. When in doubt, get seen.
References
-
Ellison P, Molloy AP, Mason LW. Early Protected Weightbearing for Acute Ruptures of the Achilles Tendon: Do Commonly Used Orthoses Produce the Required Equinus? Foot Ankle Int. 2017;38(11):1300-1305. PubMed
-
Collins R, Sudlow A, Loizou C, Loveday DT, Smith G. Closing the gap on Achilles tendon rupture: a cadaveric study quantifying the tendon apposition achieved with commonly used immobilisation practices. Foot Ankle Surg. 2018;24(2):124-127. PubMed
-
Qureshi SA, Ibrahim T, Rennie WJ, Furlong AJ. Dynamic Ultrasound Assessment of the Effects of Knee and Ankle Position on Achilles Tendon Apposition Following Acute Rupture. J Bone Joint Surg Am. 2011;93(24):2265-2270. PubMed
-
Diniz LO, Pacheco FS, Guerra-Pinto F, et al. Achilles tendon elongation after acute rupture: is it a problem? A systematic review. Knee Surg Sports Traumatol Arthrosc. 2020;28(12):3982-3991. DOI: 10.1007/s00167-020-06010-8
-
Silbernagel KG, Steele R, Manal K. Deficits in Heel-Rise Height and Achilles Tendon Elongation Occur in Patients Recovering from an Achilles Tendon Rupture. Am J Sports Med. 2012;40(7):1564-1571. DOI: 10.1177/0363546512447926
Primary source: Ellison P, Molloy A, Mason LW (2017). Early Protected Weightbearing for Acute Ruptures of the Achilles Tendon: Do Commonly Used Orthoses Produce the Required Equinus?
