If you have just torn your Achilles tendon, it is normal to feel hyper-focused on re-rupture — a second snap is scary, easy to picture, and often what friends warn you about. In modern pathways, re-rupture rates are relatively low (commonly quoted around 3–5% when people follow treatment). At the same time, tendon elongation — the tendon healing in a longer, slacker position — shows up much more often on imaging and is the issue surgeons and physios worry about when they talk about push-off power, heel-rise height, and return to sport. This article compares the two problems in patient language, explains why protocol-led early movement still makes sense, and links to deeper guides on boots, wedges, and long-term strength.
Contents
- Key takeaways
- What is re-rupture?
- What is tendon elongation?
- Side-by-side: how the risks differ
- Why early rehab feels like a balancing act
- What research suggests
- What this means for your recovery
- Frequently asked questions
- References
Key takeaways
- Re-rupture after Achilles rupture is uncommon overall (often cited around 3–5% with modern care) but serious when it happens — early months need real protection.
- Tendon elongation (healing “long”) is much more common on scans and is linked more clearly to biomechanics (how the tendon behaves under load) than to every questionnaire score — symptoms still vary person to person.
- The goal of boot angle, wedge removal, and night protection is not to ban movement — it is to keep dorsiflexion (toes-up) and load inside what that week’s healing tissue can tolerate.
- Protocol adherence and gradual progression remain the main levers you control: do not advance wedges or hinges early, avoid aggressive calf stretching in the vulnerable window, and use supervised rehab to rebuild strength without corner-cutting.
- Warning signs after a slip, trip, or forced stretch — new pop, sharp change in symptoms, unable to trust the leg — warrant urgent review.
What is re-rupture?
Re-rupture means the healing tendon tears again. It is the “back to square one” complication patients picture first.
- What it feels like: often a sudden snap or pop, sharp pain, and immediate loss of confidence in pushing off — but pain levels can vary, so do not rely on drama alone.
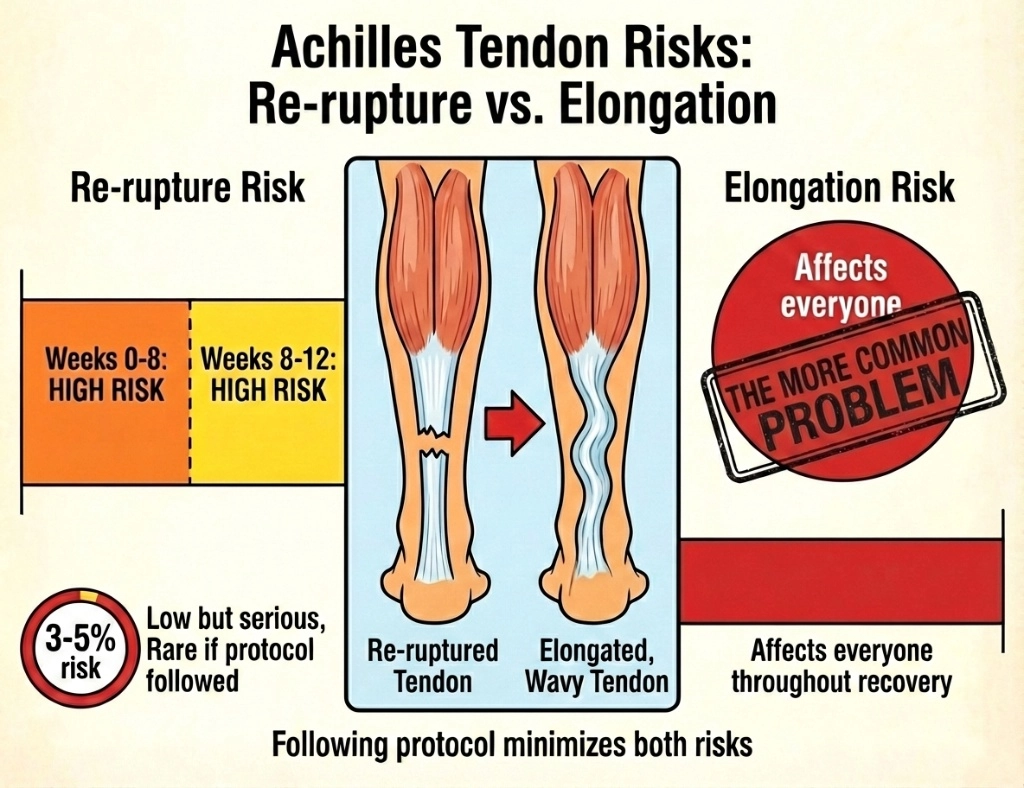
- When risk is discussed most: teams usually emphasise care in the first weeks to months while the new tissue is still maturing — your infographic’s weeks 0–12 “high attention” idea matches how cautiously people are asked to move while the repair is vulnerable.
- Big picture rate: in many modern series and summaries, overall re-rupture sits in the low single digits — low enough that many people will never see it, high enough that sloppy boot use or unprotected dorsiflexion is never worth the gamble.
If you want a hour-by-hour mindset for the very first days, see first 24 hours after Achilles rupture; for the full pathway, our recovery timeline pulls appointments, boots, and milestones into one place.
What is tendon elongation?
Tendon elongation means the repaired muscle–tendon unit ends up longer than ideal — the tendon may still be continuous, but it behaves like a looser rope. Clinicians sometimes call this healing “long.”
- Why it matters mechanically: a longer Achilles can shift where the calf works best at the ankle, which helps explain why some people track lower single-leg heel rises, less “spring” when walking fast, or limits at high-level sport even when day-to-day life feels fine.
- Not the same as “failed healing”: many people with some imaging lengthening still return to work, running, and sport. The link between millimetres on ultrasound or MRI and how you feel is not one-to-one.
- Different from normal thickening: a lump or thicker tendon under the skin is common after healing and not the same question as length — if you are unsure what changed on your scan, ask your team to show you what they measured.
For a deeper dive on strength tests and long-term numbers, read long-term strength after Achilles rupture.
Side-by-side: how the risks differ
| Topic | Re-rupture | Tendon elongation |
|---|---|---|
| How patients picture it | Another snap; “I tore it again” | The tendon heals but stretches; push-off feels weaker or “flat” |
| Typical scale in studies | Often summarised around 3–5% long-term re-rupture with modern protocols | Imaging lengthening is common; how much it hurts sport varies by person and demand level |
| Time course | An event — usually a mistake (fall, forced stretch, boot off too early) or bad luck | A process — weeks to months of healing under how you load and protect the ankle |
| What helps | Protected position, boot discipline, no unplanned dorsiflexion, urgent review if red flags | Exact wedge/hinge schedule, no rushing angles, progressive loading, avoid aggressive early stretching |
| What is misleading | Assuming “I’m safe now” too early | Assuming every millimetre on a scan dictates pain or performance |
Why early rehab feels like a balancing act
Good modern care is not “freeze the leg for months.” Many protocols use early weight-bearing in the boot, protected walking, and physiotherapy starting around weeks 3–6 — but the type of movement matters.
- Helpful early movement: Walking in the boot as allowed, muscle activation your physio prescribes, hip and knee control work, gradual load that respects your allowed ankle angle.
- Risky early movement: Barefoot walking before clearance, removing heel wedges early, pushing the ankle upward to “stretch,” long stride or steep hills that force dorsiflexion, or sleeping with the foot flopping up without a plan.
That is the Goldilocks idea from your social post: too aggressive too soon may encourage length change in immature tissue; too timid can mean stiffness and deconditioning — but fixing fear by breaking boot rules is the option that creates re-rupture risk. The through-line is control, not maximal hurry.
Practical tools on the site that match this mindset:
- Achilles tendon healing and early protection — why weeks 3–6 matter for bridge tissue
- Boot wedge removal protocol — why schedules are not negotiable DIY items
- Foot position in Achilles recovery — plantarflexion vs dorsiflexion in plain English
- Aircast vs VACOped — brand matters less than how you use whatever you were given
If nights are when you struggle to keep the foot safe, many teams discuss a dedicated Achilles night splint once it fits your phase of care.
What research suggests
-
Elongation is measurable in many patients. A 2020 systematic review pooling imaging studies found mean Achilles lengthening from about 0.15 cm to 3.1 cm depending on the cohort and measurement method. It reported fair evidence that elongation influences biomechanical outcomes, while patient-reported scores and simple strength tests did not line up with elongation as consistently — in other words, science backs “this is real on a force plate” more than “every longer tendon feels awful.”
-
Re-rupture remains a low headline number for many modern programmes, not zero. Recent meta-analyses comparing non-operative and operative care still find low absolute re-rupture rates and mostly trade-offs between other risks — another reason rehab quality and compliance dominate real life more than forum myths.
-
How you load during early functional rehab changes muscle and tendon geometry. Prospective cohort work on early functional mobilisation after repair shows details of the loading programme can influence tendon length markers and calf muscle over time — supporting the idea that controlled progression is neither “nothing” nor “anything goes.”
-
Clinical targets you can train toward — high-quality single-leg heel raises, symmetry, hop and run criteria — remain central in modern return-to-sport thinking; see our course if you want a structured, patient-friendly programme alongside your local team.
What this means for your recovery
- Keep the scary complication in perspective: re-rupture is rare, not impossible — use your boot and crutches exactly as prescribed, and do not “test” the tendon barefoot.
- Respect the quiet complication: assume some length change can happen unless you protect position — treat angle progression like a prescription.
- Do not substitute Dr Internet for your protocol: if two websites disagree, your fracture clinic wins.
- Build strength without corner-cutting: work with your physio on progressive calf loading; avoid aggressive stretching early in recovery — our clinical line is no forced aggressive stretch until the tendon is mature, often talked about as 12–18 months for hard stretching goals.
- Screen for urgents: new pop, step-off weakness, severe pain after a stumble, calf pain with breathlessness → seek emergency care.
Frequently asked questions
Is re-rupture or tendon elongation the bigger worry after Achilles rupture?
Re-rupture is the dramatic emergency patients often fear first — overall it is uncommon (often quoted around 3–5% with modern protocols). On imaging, measurable tendon lengthening after rupture is much more frequent, and evidence links it more consistently to biomechanical measures than to every symptom questionnaire. In plain terms: elongation is the common, quiet issue; re-rupture is the rare, loud one.
Does everyone’s Achilles tendon heal “too long”?
Many studies report some increased tendon length after rupture treatment. The 2020 systematic review noted mean imaging-measured lengthening from about 0.15 cm to 3.1 cm across summarised studies — but symptoms and strength do not line up neatly with millimetres. Plenty of people function well despite measurable lengthening; others notice push-off or heel-rise limits. Your team weighs scans, examinations, and strength tests together.
What increases elongation risk in early rehab?
The usual theme is toe-up (dorsiflexion) or load before your protocol permits it — speeding up wedge or hinge progression, aggressive calf stretching, walking without the boot, sleeping without agreed night protection, or long steps / hills that force the ankle upward. Start from your own schedule; for the fragile bridge weeks, see Achilles tendon healing and early protection.
How do I protect length without becoming “too cautious”?
Modern care commonly includes early weight-bearing in the boot as tolerated, physiotherapy from roughly weeks 3–6, and gradual boot weaning — movement is not the enemy. Uncontrolled dorsiflexion is. Use protected walking, respect wedge removal, use heel lifts when transitioning out of the boot if advised, and build calf strength progressively with your physio.
When should I seek urgent help?
New pop or snap, sudden giving way, sharp pain after a specific incident, rapidly worsening swelling, calf pain with breathlessness, or chest pain need urgent medical review — re-rupture and blood clots are uncommon overall but serious. If unsure, get checked.
References
-
Diniz LO, Pacheco J, Guerra-Pinto F, et al. Achilles tendon elongation after acute rupture: is it a problem? A systematic review. Knee Surg Sports Traumatol Arthrosc. 2020;28(12):4011-4030. DOI: 10.1007/s00167-020-06010-8
-
Silbernagel KG, Steele R, Manal K. Deficits in Heel-Rise Height and Achilles Tendon Elongation Occur in Patients Recovering from an Achilles Tendon Rupture. Am J Sports Med. 2012;40(7):1564-1571. DOI: 10.1177/0363546512447926
-
Aufwerber S, Edman G, Grävare Silbernagel K, Ackermann PW. Changes in Tendon Elongation and Muscle Atrophy Over Time After Achilles Tendon Rupture Repair: A Prospective Cohort Study on the Effects of Early Functional Mobilization. Am J Sports Med. 2020;48(13):3296-3305. DOI: 10.1177/0363546520956677
-
Deng H, Cheng X, Yang Y, Fang F, He J, Tian Y, et al. Rerupture outcome of conservative versus open repair versus minimally invasive repair of acute Achilles tendon ruptures: A systematic review and meta-analysis. PLOS ONE. 2023;18(5):e0285046. DOI: 10.1371/journal.pone.0285046
-
Massen FK, Shoap S, Vosseller JT, et al. Rehabilitation following operative treatment of acute Achilles tendon ruptures: a systematic review and meta-analysis. EFORT Open Rev. 2022;7(10):680-691. DOI: 10.1530/EOR-22-0072 (PMC free article)
Primary source: Diniz LO, Pacheco J, Guerra-Pinto F, et al. (2020). Achilles tendon elongation after acute rupture: is it a problem? A systematic review
