Walking without the boot after Achilles rupture is a huge psychological milestone—but it is also where mechanical demands jump. Many teams call this broader window Phase 2 rehabilitation: you are moving from protected recovery toward normal walking forces. The right question is usually not “what week is it?”, but whether your calf and tendon can tolerate the loads of unprotected gait.
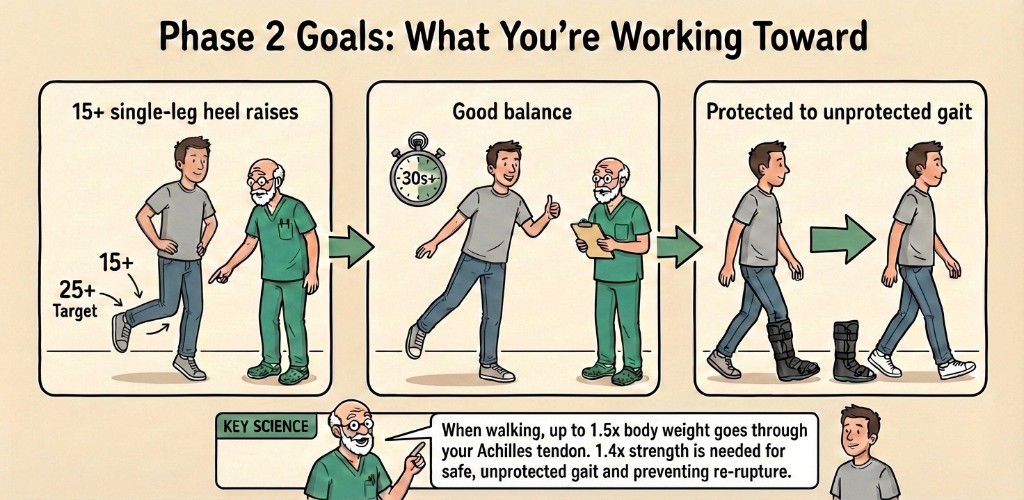
This article explains the “load case” behind that decision, the strength and balance targets you often see on patient graphics (including 15+ toward 25+ heel raises, ~30 seconds single-leg balance, and the idea of ~1.4× body weight plantarflexor capacity in some specialist teaching), and why rushing can feed tendon elongation and long-term calf weakness. Pair it with when the walking boot comes off (often discussed around weeks 10–12 using criteria) and early loading context in week 6 seated calf raises.
Contents
- Key takeaways
- Why walking is a bigger load jump than it feels
- Strength targets: heel raises and calf capacity
- Balance and gait quality
- What can go wrong if you progress too early
- What this means for your recovery
- Frequently asked questions
- References
Key takeaways
- Unprotected walking after Achilles rupture is strength-led, not calendar-led: your tendon must tolerate repeated push-off loading.
- Teaching infographics often quote ~1.5× body weight as a simple load anchor; research numbers vary by speed and measurement, but the theme is consistent: walking is not “gentle” for the Achilles.
- Single-leg heel raises are a common functional test: 15+ repetitions can appear as an early Phase 2 checkpoint, while about 25 reps is a commonly cited fuller target elsewhere on this site—with technique and symmetry mattering as much as counting.
- Single-leg balance (for example 30+ seconds) helps show you can control the leg through stance, not only move it.
- Progressing too early can worsen tendon elongation, limp, and long-term push-off power—if load races ahead of capacity, the tendon may heal longer, not just “faster.”
Why walking is a bigger load jump than it feels
When you walk, the Achilles is loaded hardest around late stance and push-off. Patient-friendly graphics sometimes summarise that as up to ~1.5× body weight per step as a rounded teaching number.
If you read biomechanics papers, you will see different multiples depending on gait speed, protocol, and whether researchers used in vivo imaging versus musculoskeletal models. For example, ultrasound-based estimates in healthy adults reported peak Achilles tendon forces around multiple times body weight during walking and higher still during running (Wiesinger et al., 2021).
You do not need to memorise the physics. The clinical headline is simpler: each step is a small hop for the calf, and removing the boot removes a layer of external support right when that load matters.
Strength targets: heel raises and calf capacity
Single-leg heel raises (15+ working toward 25+)
Repeated single-leg heel raises test whether you can produce and repeat plantarflexion force through the recovering tendon—similar to what walking demands thousands of times per day.
Graphics often show “15+” as a first functional band and “25+ target” as a next band. On Thetis we align the long-range aim with other articles: about 25 high-quality single-leg heel raises is a widely used modern rehabilitation anchor for higher-level activity—but only when your team clears it, and never as a DIY race.
Technique beats bragging rights:
- Rise straight up, not rolling onto the little toe.
- Use a wall or finger touch for balance if needed at first—your physiotherapist will spell out what counts as “assisted” versus “clean.”
- Compare side-to-side height and fatigue; many people can hit a rep count while still protecting subtly.
Isometric plantarflexion and the “~1.4× body weight” idea
Some rehabilitation teaching references an isometric plantarflexion strength benchmark in the region of ~1.4× body weight when discussing capacity for unprotected gait and guarding against re-injury.
In real-world NHS and community physio, most patients will not undergo formal dynamometry like a research lab. If your programme includes handheld dynamometry, force plates, or similar, treat the number as context from that setup—not something to “score” at home.
Balance and gait quality
Single-leg balance (~30+ seconds)
Standing on the injured leg sounds basic, but it catches ankle strategy, hip control, and fear-driven offloading that make people hike the hip, shorten steps, or turn the foot out. Those patterns can nudge uneven loading through the tendon.
A 30+ second stance target (as shown on many patient visuals) is simply a practical screen for baseline control before you expect the leg to carry you all day.
“Protected to unprotected gait”
Readiness is rarely one number. Experienced clinicians blend:
- Pain and irritability rules (symptoms that spike for hours after activity),
- Strength tests (heel raises, weighted progressions),
- Movement quality (smooth push-off, calf usage, not collapsing into valgus),
- Your specific protocol (operative vs non-operative, speed goals, work demands).
For a wider rehab map, browse Achilles rupture rehabilitation FAQs and the structured lessons in our Achilles recovery course.
What can go wrong if you progress too early
If you walk unprotected before the calf can brake and propel cleanly, the body often compensates:
- Shorter steps and less ankle push-off,
- Early timing onto the other leg,
- Hip hiking or turning the foot outward.
Those strategies can allow more tendon strain in subtle ways, and they are associated in the literature with outcomes people feel long term: tendon elongation, lower heel-rise height, and asymmetry (Silbernagel et al.; later follow-up work links heel-rise height deficits to lasting gait changes).
None of this means you should be scared to progress when your team clears you. It means criteria exist for a reason.
What this means for your recovery
Do:
- Ask your physiotherapist which specific tests gate your boot weaning and shoe walking in your protocol.
- Film a short walking clip (side and behind) when your team asks—small form issues are easier to spot on video.
- Keep heel lifts and gradual weaning if your clinician prescribes them—abrupt “zero support” days are not a badge of honour during transition.
Avoid:
- Chasing rep counts with ugly technique (bounding, pain grimace, collapsing).
- Aggressive dorsiflexion stretching to “loosen the ankle for walking” early on—our site-wide stance is to avoid aggressive stretching until much later healing (tendon maturity), matching your clinician grading.
- Quietly doubling daily steps because you feel impatient—volume jumps are how irritability flares appear.
If push-off suddenly feels wrong, the calf clunks, or pain spikes—treat that as a signal to slow down and get same-day advice if severe.
Frequently asked questions
How much load goes through the Achilles when I walk?
Everyday walking loads the Achilles heavily at push-off. Exact multiples of body weight vary with speed, shoes, and measurement method: some in vivo studies report peak Achilles tendon loads on the order of roughly 2–3 times body weight during walking, while musculoskeletal models sometimes predict higher peaks. Infographics often summarise with a round number like ~1.5× as a teaching anchor. The practical point is the same: ditching the boot is a real load jump, which is why clinicians lean on strength-led criteria rather than dates alone.
What do 15 versus 25 single-leg heel raises mean?
Repeated single-leg heel raises are a simple bedside check of calf endurance and control. Many pathways use lower rep targets as an early functional checkpoint, then build toward higher rep targets—on this site we treat about 25 single-leg heel raises (with good technique) as a commonly cited gold-standard style milestone for higher-level activity, but timing is always criterion-based and your physiotherapist sets the target. Quality (height, symmetry, no cheating) usually matters more than the exact number on day one.
What is the ~1.4× body weight strength idea on some graphics?
Some teaching materials reference a plantarflexor strength level in the ballpark of body-weight multiples (often shown around ~1.4×) when discussing safe unprotected gait. In routine NHS care, most patients never get lab-grade force testing like that in a graphic; teams instead use practical tests (heel raises, calf raises on a step, balance, gait quality, hop progressions when appropriate). If your programme uses dynamometry, interpret the results with the clinician who measured them.
Why is single-leg balance part of boot-to-shoes readiness?
Walking is thousands of single-leg moments. If you cannot stand steadily on the injured leg, you are more likely to hitch, twist, shorten the step, or offload awkwardly—patterns that can encourage tendon elongation and a limp that sticks. Targets like 30+ seconds of controlled single-leg stance are a simple way to screen control before you rely on the tendon for full-day loading.
What if I progress before I am strong enough?
Pushing into unprotected walking too early can contribute to the tendon healing in a more lengthened position (tendon elongation), a residual limp, weaker push-off, and higher re-injury risk. If pain sharply rises, the calf feels unstable, or gait becomes markedly uneven, step back and speak to your fracture clinic or physiotherapist sooner rather than pushing through.
Is Phase 2 always the same dates for everyone?
No. Phase labels differ between hospitals. What matters is meeting the functional tests your team sets, often alongside gradual boot reduction—commonly discussed around weeks 10–12 when criteria are met (see walking boot removal timing).
Do I need dynamometry to leave the boot?
Most people do not. Practical strength and gait tests dominate community care. Dynamometry is optional where available.
How does this tie to running later?
Running is another load jump. Return-to-run plans usually wait for stronger milestones—often higher-quality calf capacity and plyometric readiness beyond normal walking—even when day-to-day steps feel manageable.
References
-
Wiesinger HF, Kösters A, Müller E, Seynnes OR. Quantifying mechanical loading and elastic strain energy of the human Achilles tendon during walking and running. Sci Rep. 2021;11:3601. https://doi.org/10.1038/s41598-021-84847-w
-
Zellers JA, Carmont MR, Grävare Silbernagel K. Defining Components of Early Functional Rehabilitation for Acute Achilles Tendon Rupture: A Systematic Review. Orthop J Sports Med. 2019;7(11):2325967119884071. https://doi.org/10.1177/2325967119884071
-
Silbernagel KG, Steele R, Manal K. Deficits in Heel-Rise Height and Achilles Tendon Elongation Occur in Patients Recovering from an Achilles Tendon Rupture. Am J Sports Med. 2012;40(7):1568-1575. https://doi.org/10.1177/0363546512447926
-
Zellers JA, Carmont MR, Grävare Silbernagel K. Heel-Rise Height Deficit 1 Year After Achilles Tendon Rupture Relates to Changes in Ankle Biomechanics 6 Years After Injury. Am J Sports Med. 2018;46(11):2670-2677. https://doi.org/10.1177/0363546517717698
Primary source: Wiesinger HF, Kösters A, Müller E, Seynnes OR. Quantifying mechanical loading and elastic strain energy of the human Achilles tendon during walking and running
